
Paul Offit on Dr' Mike
Is there a Fauci syndrome present?

So in Dr. Mike’s video
dr Paul Offit pretty confidently referenced this study at minute 43: https://jamanetwork.com/journals/jamacardiology/fullarticle/2780548 in the video interview, to claim that incidence of myocarditis from covid in young athletes is 2.5% or “one in 45”?!?
Number sounds unrealistically high, doesn’t it?
Let’s look into it with some nuance…
In the study they analyzed 1597 athletes from “big 10” that tested positive for symptomatic covid and were tested for myocarditis afterwards.
There are “few problems” with this study and dr Offit interpretation:
1.No baseline (same athletes were not tested before to establish baseline, if some of them had condition before symptomatic covid and myocarditis evaluation, which in normal studies are subtracted/excluded from difference (hence baseline)
2. Symptomatic covid cases only are a form of case cherry picking, a common problem which leads to base rate fallacy.
3 Case definition was very loose and ambiguous that even had major groups with description like “probable” and “possible”!
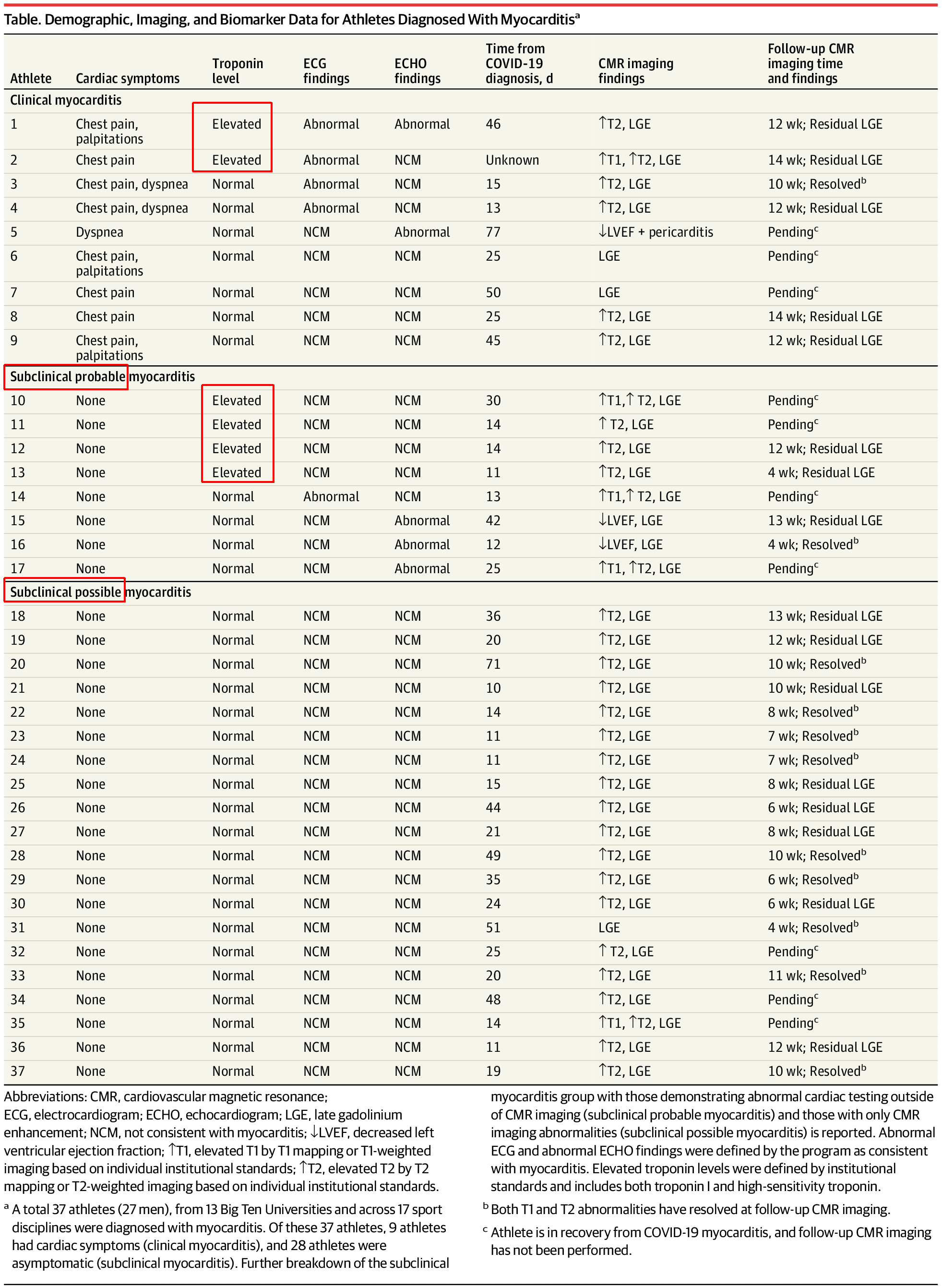
3.1 “Cardiac enzymes on everybody” as dr Offit stated were not detected as elevated on all “myocarditis cases”, only 0.3% had elevated Troponin, but that one falls on Offit’s (faulty) interpretation of the study results (6 not 37).
Now, remember marine study from our previous article?
Looks like in the Marine study which tested ALL the Marine recruits in a very regular fashion (no cherry picking), symptomatic and asymptomatic covid cases were detected and recorded.
In 9.8% of total covid cases detected, only 5 of 51 was found to be symptomatic, which when applied as proper denominator reduces prevalence by roughly almost 10 times unless we test everybody.
In big 10 study table it was even classified other cases as subclinical, probable, and subclinical possible myocarditis:
It turns out if we correct for base rate fallacy, out of 1597 athletes , 37 had “clinical, subclinical possible and subclinical probable” myocarditis (2.3%) out of which just 6 had elevated troponin levels.
Troponin is gold standard in detecting heart damage. As noted in: https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.107.722975 “Cardiac troponin (cTn) has established itself firmly as the “gold standard” in the diagnosis of ACS “
On top of all this there is huge problem of case classification, apparently if we adjust for all covid cases and not only symptomatic as per Marine study range of cardiac effects shifts from 0.23% for all cases including “subclinical probable and subclinical possible” and to 0.03% of troponin positive cases. Only one assumption is made, that non symptomatic cases were also not influencing cardiac function which is way more reasonable then assuming that it does as it was implied by paper authors and dr. Offit based on their interpretation (bias is clear).
What follows is data backed approximation and comparison:
Is there better study to compare with vaccinated youth?
Thai study ! that was also commented by cardiologist Anish Koka in his subsstack
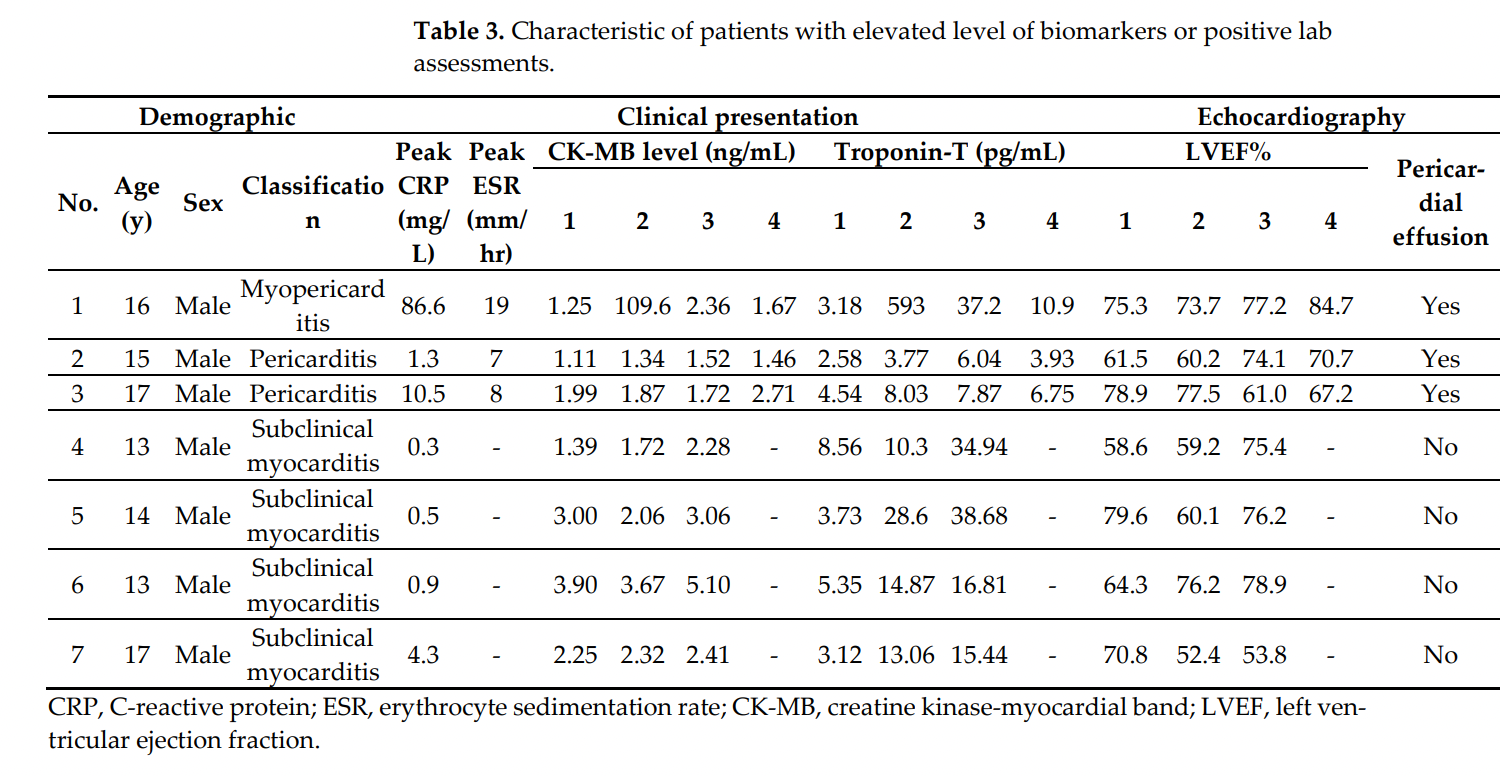
In this study 300 kids was tested prior to vaccination to establish baseline (+1 all tested for baseline, way better study design then big 10 study that Offit referenced), and they re-tested ALL the vaccinated kids post vaccination again (+2 testing all the kids not just symptomatic removes second shortcoming ) also they focused on clinical confirmation based on elevated troponin levels (+3) so it is vastly better designed study to be used for comparison!
What did they find?
Unfortunately 7 kids out of 300 (2.3%) had elevated troponin post vaccination, or heart damage confirmed with gold standard diagnostic!
Lets calculate the ratio for those two studies
So for definitive heart damage problem confirmed with troponin test, big 10 had 0.03-0.3% cases ranging from adjusted cases for all probable cases, to confirmed symptomatic-elevated troponin confirmed cases.
While Thai study had 2.3% of kids with troponin confirmed cases (4 were subclinical). far cry from dr Offits quoted CDC’s number 1 in 6600 in that age group?! Looks like URF in vaccine caused myocarditis in teen age group case is 153x!!
Ratio of harm from vaccine outweighs myocarditis from covid by factor of 7.6 to 76.6 times, if we compare apples to apples (troponin positive cases only) it is 76.6 times more likely kids will have myocarditis with elevated troponin (gold standard) from these two studies alone adjusted for denominator error!
Only by few researchers came close to this like Vinay Prasad in article https://brownstone.org/articles/myocarditis-under-age-40-an-update/ even that ratio is lacking due to the underreporting problem and other problems I already mentioned above.
Vinay also discusses clearly identified under-reporting problems due to misclassification of the cases stemming from wrong ICD reporting codes, large time delays in reporting or just plain underreporting due to physicians simply not reporting those cases, that was identified by dr. Katie Scharff and discussed in fine detail:
dr. Scharff with dr. Prasad on his youtube channel:
Dr. Scharff also published these findings in her paper: https://www.ajconline.org/article/S0002-9149%2822%2900192-8/fulltext
Now in post DB-RCT gold standard studies, in vaccine monitoring there is heavy skew present, or under-reporting factor (URF) that plagues VSD/VAERS systems that ranges from only 1% of cases reported (based on Lazarus report) (equates to ~100x URF) all the way to i.e. Anaphylaxis prevalence of 2.1%, ratio identified in https://jamanetwork.com/journals/jama/fullarticle/2777417 compared to CDC original rate of 2.5-11.1 cases per milion (CPM) compare that to 210CPM in paper, URF ratio that range from 18.9-100times difference tells you something is wrong with reporting system!
Basically URF is clearly identified and ratio is huge!
Largest problem in todays medical community is Medical Gaslighting!
https://www.psychologytoday.com/us/blog/navigating-cancer/202209/dealing-medical-gaslighting , which is glaring if you see most of the testimonies of vaccine injured, it is common occurrence and explains some of the systematic biases due to physicians being biased, and ill advised from three letter agencies to ignore these effects as improbable based on flawed statistics.
Now why article has reference to Fauci effect?
When some powerful and influential person twists information to conform it’s biases, when presented with truthful or different information there are several response pathways, one very popular is “attack on me is attack on science”, famous quote form dr. Fauci
How person reacts to presentation of data and interpretation is pretty telling, if it reacts with scrutiny, that is desirable, if presentation has flaws. If there is agreement and there is no observable flaws in analysis that is also ok. If it attacks back with strawman+ad hominem, but no substance or argument- you have Fauci syndrome at hand!
We completed the picture here, but will attack this problem with more concrete evidence based science from yet another angle!
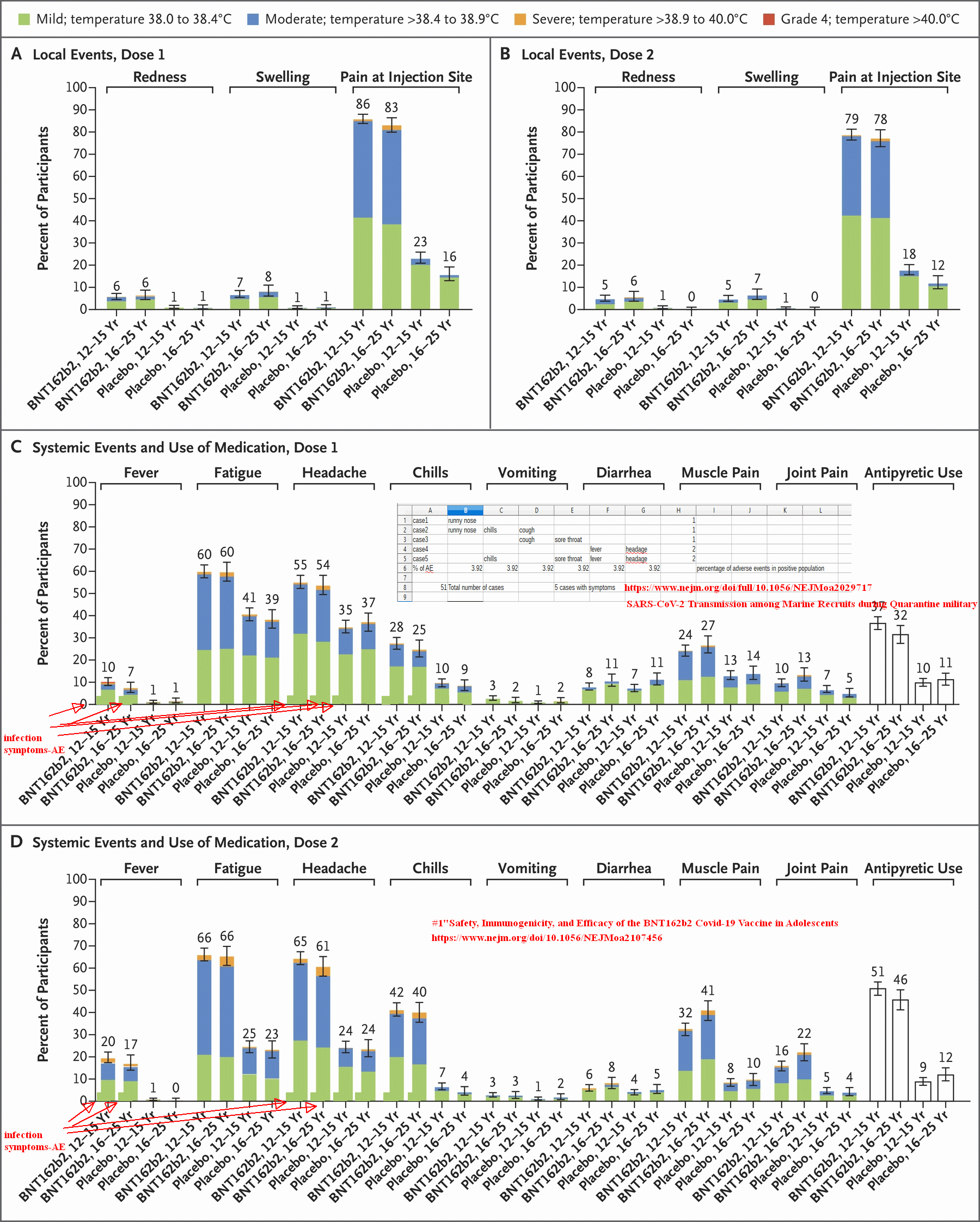
I already mentioned Marine study which leaves very little room for bias, very solid science behind it, we can overlay covid adverse events data from marine study with “Gold standard” prospective, Double blind, randomized, placebo controlled trial ( Safety, Immunogenicity, and Efficacy of the BNT162b2 Covid-19 Vaccine in Adolescents ), as adverse effects of vaccine teenage recipients vs covid infected recruits in marine study which are also athletic teens.
What do we see here?
Lets pull data out and calculate comparative ratio for matching available outcomes.
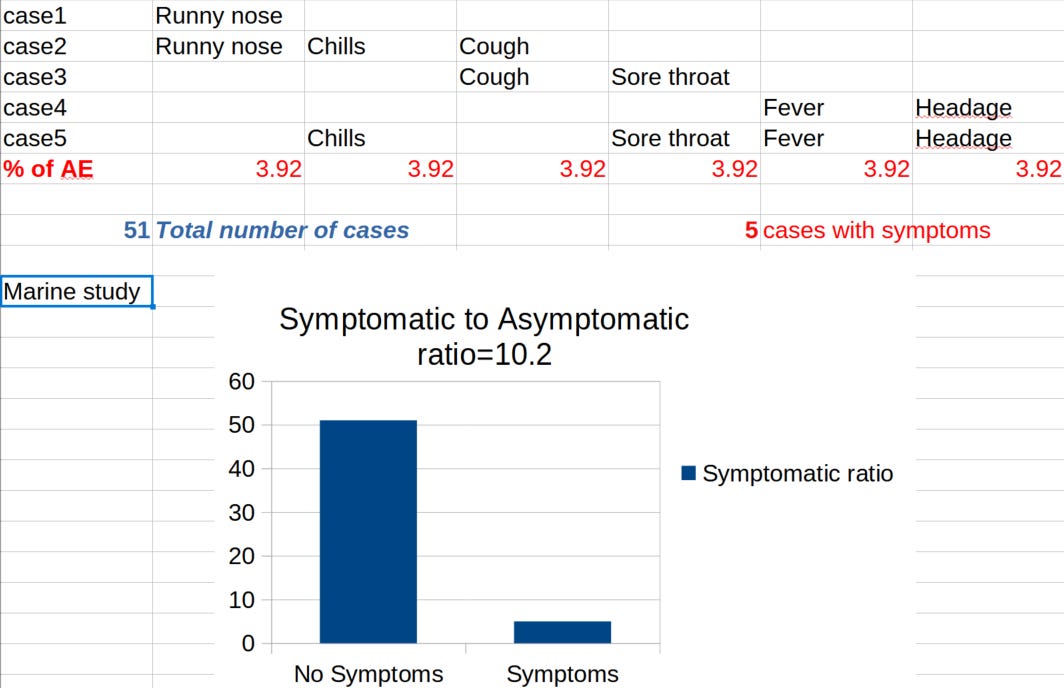
In marine study there was 51 cases of covid, 5 with symptoms.
Let’s compare covid caused same symptoms or adverse events (AE) and vaccine EUA study for teens.
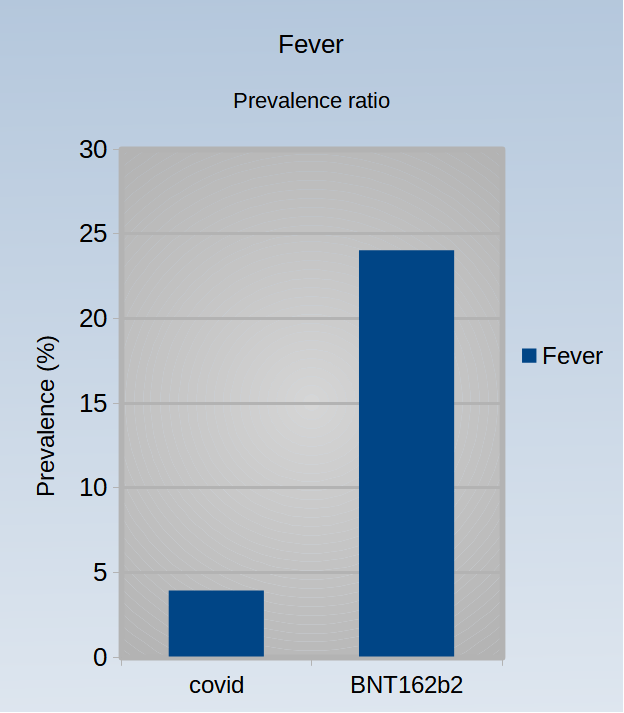
In Marine study there was 3.9% prevalence of Fever, while in Vaccine study that prevalence was 7% for first dose and 17% for second dose, so you experience AE two times or cumulative of 24% compared to 3.9% which gives odds ratio of 6 times more likely to have fever from vaccine then from covid in study group p=0.002349!
Other AE’s are way more likely, to experience headage from covid in marine study had prevalence of only 3.9% again, in EUA 54+61% which gives ratio of 30x p=0.000002 FOR 54% and for 61% p=0!
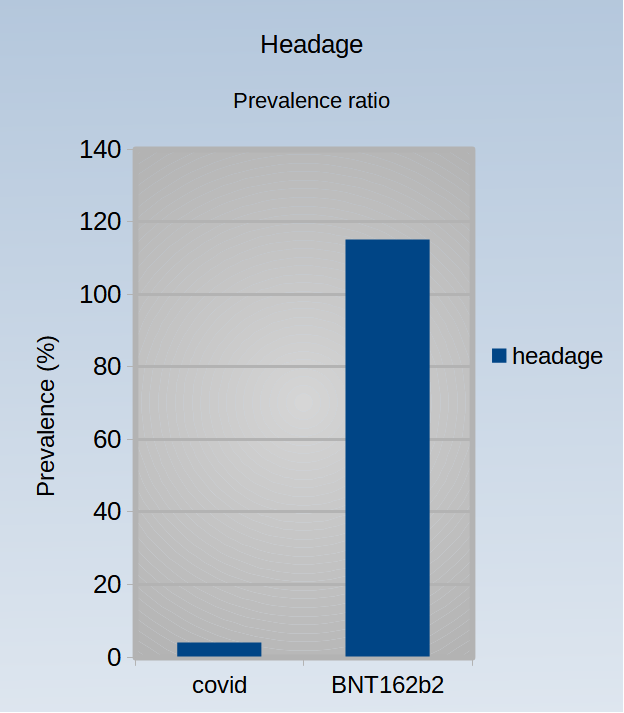
Cumulative prevalence is 115% since you experience headage AE twice(51+64)
Chills 3.9% vs 25+40% or 16x p=0.001860 for 25%
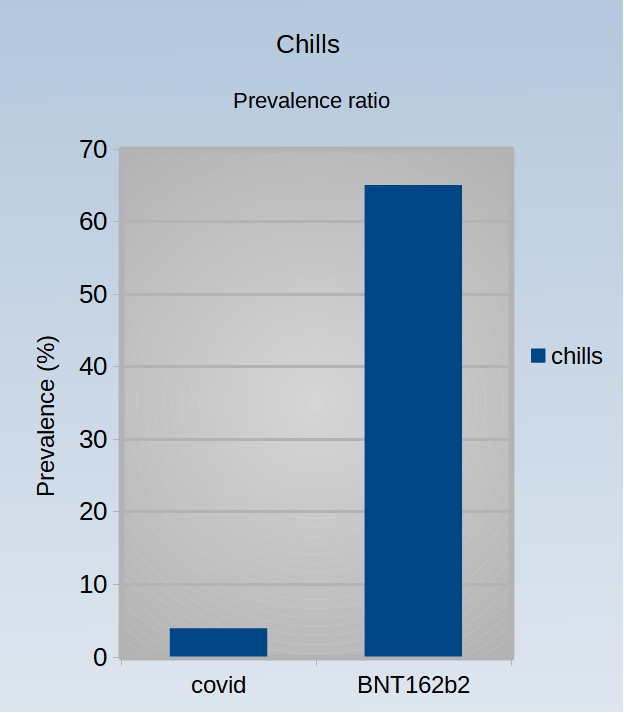
16 times higher likelihood of experiencing chills from vaccine, then from actual Covid!
These latter results are in agreement with fist comparison that was done by correcting for problems in the study! That does not make any sense! Also Why is marine study chosen, because there is no bias that is only study that caught all the cases because of super study design, ALL other studies except for prospective DB-RCT’s are faulty!
From this multi angled comparison it is obvious that when you don’t have denomination error, or some other confounder, and situation is clear (all cases are included-no cherry picking) it is pretty clear to see how vaccine caused adverse events actually surpasses even covid caused AE by a large margin!
Looks like in any metric AE from vaccine is larger then AE from covid in same age group, personally this looks like we are preparing for head knock from 3”foam ball (covid), “training” it while hitting head with baseball bat-full swing (vaccine)!
Problem is in case of dr. Offit, to know these things, that is his job, bread and butter, he SHOULD know this information, and he still choose to present very distorted picture by cherry-picking one study that is very lacking, and mispresenting data and conclusions in that study while keeping pretty confident posture! I doubt that he is not familiar with this information, i would fee relief if he really did not know this, then his comment would be needed!
Even results in the study he referenced are described under question mark (probable, possible…so many if’s), yet dr Offit choose to present same data as “definitive cases” of myocarditis, inflating a little even that number, look at the pasted table and what it is saying?!
Do we see Fauci syndrome here?
Is Paul Offit right?
I sure hope for constructive! criticism of this evaluation in the comments! Please point to any problems or inaccuracies so they can be corrected!
Thank you for reading
https://www.ahajournals.org/doi/full/10.1161/CIRCULATIONAHA.122.059970
" In men younger than 40 years old, the number of excess myocarditis events per million people was higher after a second dose of mRNA-1273 than after a positive SARS-CoV-2 test (97 [95% CI, 91–99] versus 16 [95% CI, 12–18]). In women younger than 40 years, the number of excess events per million was similar after a second dose of mRNA-1273 and a positive test (7 [95% CI, 1–9] versus 8 [95% CI, 6–8])."
In this study ratio for <M40yo was larger by factor of 6x post vaccination vs post covid...
I forgot about two large biases and will update text accordingly in a few days.
"Athletic bias" post viral exercise that is physically strenuous is no no, not just in case of covid, but nature of these students is to be athletic and exercise, it is also reason of their admission, so likelihood of athlete to have heart problem because of their post viral behavior is increased, how much, 2x...5x? i don't know, if someone can untangle this bias, please comment. This bias direction is forward to increase incidence of heart related problems in this study in comparison to normal student population.
Another bias is in Thai study, parents of kids involved were more vaccine friendly, plus once you make decision to vaccinate your kid, likelihood of reporting problems that will counter your previous decision is smaller, this bias is also known as https://en.wikipedia.org/wiki/Escalation_of_commitment.
So focusing on troponin only for comparison purposes makes most sense. Even though in the study there was more reported issues (22 cases of arrhythmia 20 cases of tachycardia etc. details in table 4) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9414075/